


Three Big Takeaways from the Senate Finance Committee’s Insulin Report
There is a lot going on in the United States right now, to say the very least.
It’s the last day of Donald Trump’s presidency, and far-right extremists and white supremacists are trying to keep him there. A new strain of COVID-19 is gaining hold that is estimated to be seven times more transmissible than the one already rampaging through communities everywhere. By the end of the day, we’re likely to have reached 400,000 people dead from the virus. More and more, the U.S. becomes a site of economic suffering, increasing political turmoil, and grief on an unutterable scale.
When the Senate Finance Committee, led by Sens. Chuck Grassley (R-IA) and Ron Wyden (D-OR), announced its investigation into insulin prices in the winter of 2019, the world seemed almost unimaginably more stable by comparison. Yet for many people with diabetes, 2019 was also a desperate year. Around the time the Committee began its investigation, you couldn’t find a box of long-acting analog insulin for under $400. Stories abounded of insulin’s punishing burden, like that of a furloughed federal worker choosing between insulin and her mortgage. Worst of all, lives were lost that year — Jada Louis, Josh Weaver, and Jesimya David Scherer-Radcliff — to name some of those we know about.
Things were urgent for the diabetes community then. When this investigation was launched, it wasn’t the action that was needed to stop those deaths. Then, it took another two years to complete, and now that we have the chance to read it, it doesn’t offer much in the way of revelations. Here are some of the major takeaways from the report.
Novo Nordisk almost cut their insulin prices in half in 2018 but decided not to.
In 2018, Novo Nordisk made pro and con lists about two things: 1.) whether to increase the price of its basal insulins and 2.) whether to cut the price of all their analog insulins in half in response to pressure from activists, press, and lawmakers.

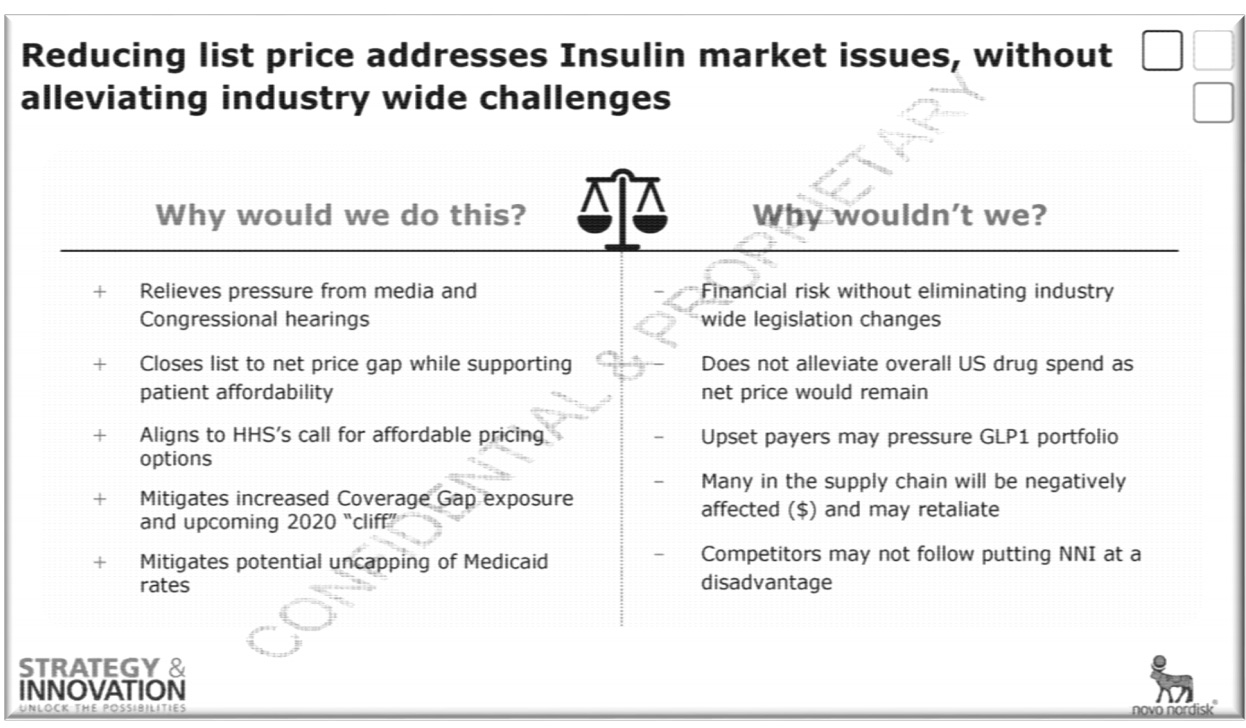
Ultimately, they did increase the costs of their basal insulins, and they decided not to dramatically cut any prices, citing fears about losing revenue, backlash from PBMs, and pressure to lower prices on other drugs. Bad PR and Congressional hearings prove no match for the financial incentives of the status quo.
Yes, PBMs incentivize driving up the list price. But manufacturers have still found a way to increase their share of revenue since the early 2000s.
The report really focuses on 2014-2018, a time when manufacturers have pointed to a relatively flat line of revenue from insulins when compared to the list price hikes. Still, when compared to the companies’ revenues going back over two decades, it’s clear the companies are still raking it in. For instance, Eli Lilly’s revenue from Humalog doubled from $1.5 billion in 2007 to $3 billion in 2018.
R&D spending pales in comparison to spending on sales and marketing.
PhRMA’s major talking point against actions like price caps or Medicare negotiation is that any loss of revenue would deter innovation down the road. PhRMA allies like JDRF have argued that while insulin affordability must be a priority, any price reductions must not come at the cost of innovation. But the report makes clear that insulin R&D really isn’t a priority for them. Less than 2% of Lilly insulin revenue goes to R&D, according to the report. Lilly made $22.4 billion on insulins between 2014-2018. During the same period, they spent $1.5 billion on sales and marketing expenses on those insulin products, and $395 million on insulin R&D.
Overall, the central narrative the report paints is one of manufacturers increasing their list prices in nearly lock step in order to offer steeper rebates to pharmacy benefit managers (PBMs) who determine their priority on insurance formularies. A version of the story has been the pharmaceutical party line for some time: we’re only making insulin expensive because this ever-so-convoluted system of PBMs and wholesalers and insurers makes us!
To be sure, there is no health justification for such restrictive insulin formularies (or for the entire system of private health insurance, for that matter) to even exist. But to say that PBMs force their hand is to understate their own complicity as the sole determinants of the price of insulin. It’s clear that at many points in insulin’s journey up to its 1200% price increase that manufacturers had to choose between their revenues and market share and the lives of the people exposed to their list prices. Over and over again they chose the former.
Small doses
Vaccine update: Three letters are calling for the CDC to update its guidance to include people with type 1 diabetes among the groups considered most at-risk for severe illness due from COVID-19. The first one came from grassroots organizations and prominent researchers, then from the American Diabetes Association, and now a correspondence in the Lancet Diabetes & Encrinology.
Blue Cross Blue Shield, PhRMA, and several pharmaceutical giants, including Eli Lilly, are among the many groups that have announced they will pause corporate contributions to Republican lawmakers who opposed certifying the results of the 2020 election. (However, it remains to be seen whether the pause will end when the time comes for actual campaigns to resume.)
The Endocrine Society released a position statement on insulin access and affordability. It largely mirrors the positions of mainstream diabetes organizations like the ADA, calling for things like price transparency in the supply chain and caps on out of pocket costs.
An interesting look at the business model of drug coupon company GoodRx in Forbes.
Maryland lawmakers managed to override the governor’s veto of establishing a state prescription drug affordability board.
The story behind the viral TikTok of a mom who said she couldn’t afford her son’s insulin.
Trump’s $200 prescription drug cards are finally here! (Er...Psych.)
Read about one of the unsung heroes of insulin’s discovery: James Collip, the one who purified the crude reduction of animal pancreas and turned it into something our bodies could handle having injected into us. Thanks for that, Dr. Collip!
Finally, a new grassroots project is set to launch soon: the Insulin Initiative. The first goal is federal insulin price caps. Pretty neat. Look for next week’s newsletter for more.


That’s all for this week’s Shot.
Inbox: theshotnewsletter@gmail.com
Twitter: @emilypisacreta
-EP